Antisense Therapy: Definition, Mechanisms, Approved Drugs, and Applications
What Is Antisense Therapy?
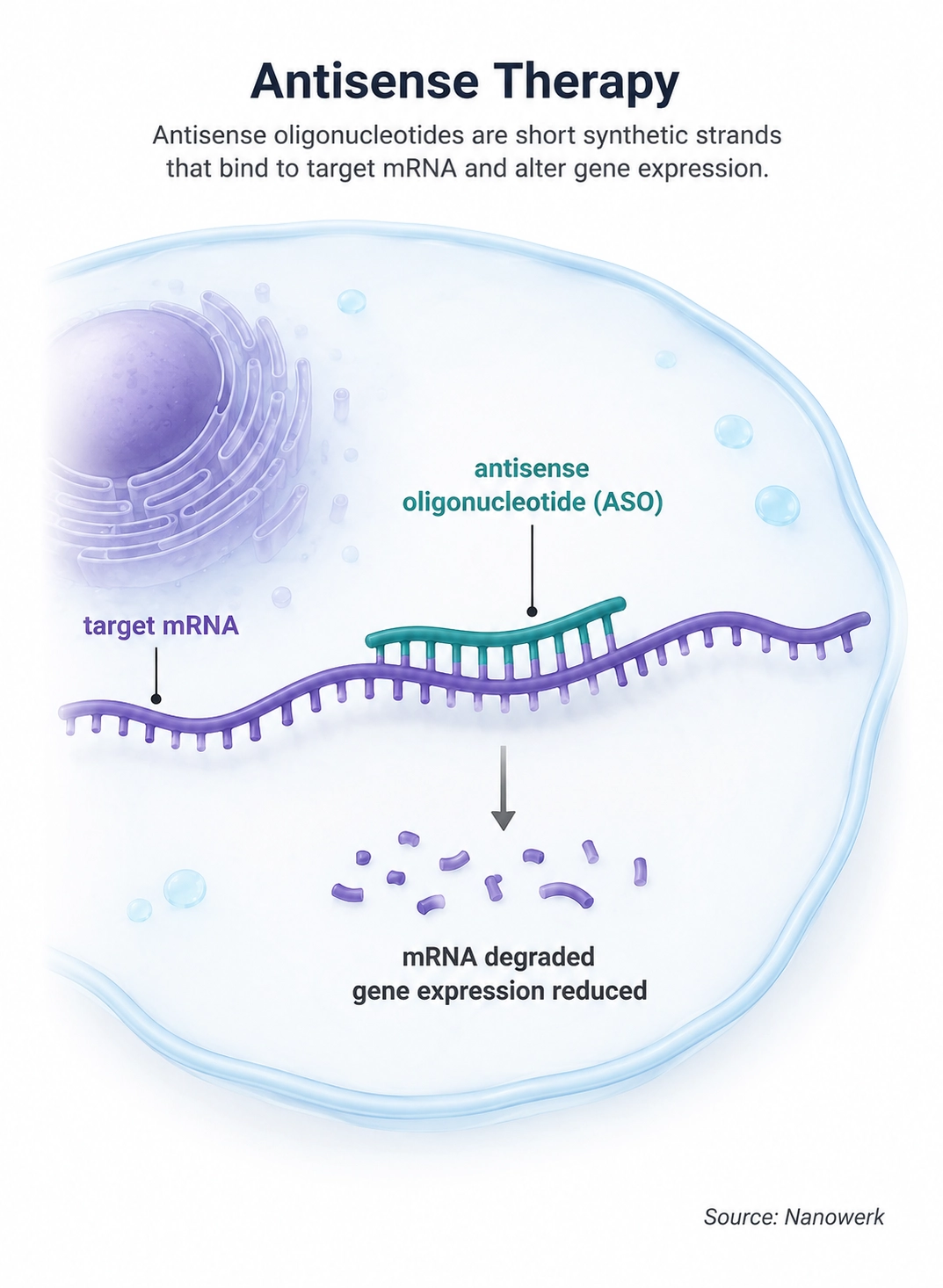
Definition: Antisense therapy is a treatment strategy that uses short, synthetic, single-stranded nucleic acids – called antisense oligonucleotides (ASOs) – to bind to a complementary RNA sequence inside cells and silence, redirect or modify the expression of a target gene.
In simple terms: instead of designing a drug to block a disease-causing protein after it has been made, antisense therapy designs a short piece of DNA-like or RNA-like material that sticks to the messenger RNA carrying the instructions for that protein. The target protein is then made in lower amounts, made in a different form, or not made at all.
Antisense therapy is one of the central modalities in modern RNA-targeted medicine. A conventional drug usually acts on a protein. An antisense drug acts one step earlier, on the messenger RNA or pre-mRNA that connects a gene to its protein product. The drug itself is an oligonucleotide, typically 15 to 25 nucleotides long, whose sequence is the reverse complement – the "antisense" – of the RNA it is meant to engage. Once the ASO finds its target, it pairs with the RNA by Watson–Crick hydrogen bonding and triggers one of several downstream effects.
In principle, many disease-related RNAs can be targeted by designing a complementary sequence. In practice, clinical feasibility depends on delivery, potency, safety, tissue distribution, RNA abundance and whether changing that RNA produces a useful therapeutic effect. As of 2026, more than a dozen antisense oligonucleotide therapies have been approved by major regulators, with most current approvals concentrated in rare genetic, neuromuscular, neurological and liver-targeted diseases. Approved examples include treatments for spinal muscular atrophy, Duchenne muscular dystrophy, SOD1-linked amyotrophic lateral sclerosis, hereditary transthyretin-mediated amyloidosis, familial chylomicronemia syndrome and hereditary angioedema prophylaxis.
At a glance:
- What it is: a class of drugs based on short synthetic single-stranded nucleic acids that bind specific RNA targets
- Typical length: about 15–25 nucleotides
- Main mechanisms: RNase H-mediated RNA cleavage, splice switching and steric blockade
- First approved ASO: fomivirsen in 1998 for cytomegalovirus retinitis in AIDS
- Recent approvals: tofersen for SOD1-ALS, eplontersen for polyneuropathy of hereditary transthyretin-mediated amyloidosis, olezarsen for familial chylomicronemia syndrome and donidalorsen for prevention of hereditary angioedema attacks
- Key advantage: the drug sequence can be reprogrammed for a new RNA target while using similar chemistry and manufacturing principles
Key Takeaways
Antisense therapy is best understood as a programmable drug platform rather than as a single treatment. By changing the oligonucleotide sequence, researchers can design ASOs to silence a gene, alter RNA splicing, skip a disease-causing exon or block translation. The same broad approach that produced nusinersen for spinal muscular atrophy can be adapted to different genes and tissues, although each candidate still requires its own testing for delivery, efficacy and safety.
The field has advanced because of chemical engineering. Unmodified DNA-like oligonucleotides are rapidly degraded in the body and enter cells poorly. Modern ASOs use backbone modifications, altered sugar chemistries, neutral morpholino structures or targeting ligands to improve stability, binding, distribution and dosing. These modifications do three main things: protect the ASO from degradation, strengthen binding to RNA and help direct the drug to useful tissues.
How Does Antisense Therapy Work?
All antisense drugs share the same first step: the oligonucleotide enters a cell, finds an RNA molecule whose sequence is complementary to it and forms a short RNA–ASO duplex. What happens after this binding event defines the main mechanisms of action used by approved antisense therapies.
RNase H-Mediated mRNA Cleavage
The most common mechanism uses a naturally occurring enzyme called RNase H. When a DNA-like ASO binds to an RNA molecule, RNase H recognizes the RNA–DNA hybrid and cleaves the RNA strand. The RNA fragment is then degraded by the cell, reducing production of the corresponding protein. Many gapmer ASOs work this way. A gapmer has a central DNA-like region that supports RNase H activity, flanked by chemically modified nucleotides that improve stability and binding affinity.
RNase H-dependent ASOs are especially useful when the therapeutic goal is to lower the amount of a toxic or disease-promoting protein. Examples include inotersen and eplontersen, which reduce production of transthyretin; tofersen, which lowers mutant SOD1 in a genetic form of ALS; olezarsen, which lowers apolipoprotein C-III to reduce triglycerides in familial chylomicronemia syndrome; and donidalorsen, which lowers prekallikrein production to help prevent hereditary angioedema attacks.
Splice Switching
Some ASOs do not destroy RNA. Instead, they bind to pre-mRNA and change how the cell splices it. Splicing is the process that removes introns and joins exons to produce mature mRNA. By masking a splice site or a regulatory sequence, a splice-switching ASO can make the cell include an exon, skip an exon or restore a more functional reading frame.
Nusinersen, used for spinal muscular atrophy, is the best-known splice-switching ASO. It binds to SMN2 pre-mRNA and promotes inclusion of exon 7, increasing production of functional SMN protein. Several ASOs for Duchenne muscular dystrophy use a related strategy called exon skipping: they cause the cell to skip selected exons in the dystrophin transcript so that a shorter but partly functional dystrophin protein can be made.
Steric Blockade
A third mechanism is steric blockade. Here the ASO binds to RNA and physically blocks another molecule from interacting with it. Depending on where the ASO binds, this can interfere with translation, alter RNA processing or prevent binding by a regulatory protein or microRNA. Steric-blocking ASOs usually use chemistries that do not recruit RNase H, such as phosphorodiamidate morpholino oligomers or 2'-O-modified oligonucleotides.
Chemistry of Antisense Oligonucleotides
The chemistry of an ASO determines much of its behavior in the body. The earliest oligonucleotides were close to natural DNA and were unstable in biological fluids. Modern ASOs are chemically modified to resist nucleases, bind more tightly to RNA, distribute to useful tissues and reduce unwanted immune activation.
The most common backbone modification is the phosphorothioate linkage, in which one non-bridging oxygen atom in the phosphate backbone is replaced by sulfur. This greatly improves nuclease resistance and increases binding to plasma proteins, extending circulation time. Sugar modifications such as 2'-O-methyl, 2'-O-methoxyethyl and locked nucleic acid increase binding affinity and stability. Phosphorodiamidate morpholino oligomers, used in several Duchenne muscular dystrophy drugs, replace the ribose-phosphate backbone with a morpholine-based neutral backbone that is highly resistant to degradation but does not activate RNase H.
A major advance has been ligand conjugation. Several newer ASOs carry a triantennary N-acetylgalactosamine, or GalNAc, ligand that binds the asialoglycoprotein receptor on hepatocytes. This directs the drug efficiently to the liver and can improve potency and dosing. GalNAc-conjugated ASOs such as eplontersen, olezarsen and donidalorsen show how tissue-targeting ligands have become central to newer antisense drug design.
Approved Antisense Oligonucleotide Drugs
Approved ASOs remain concentrated in serious diseases with strong genetic or RNA-level rationale. Some reduce toxic proteins, some change splicing and some skip exons. The table below lists representative approved antisense oligonucleotide drugs and closely related splice-switching oligonucleotides. Approval status varies by country and continues to evolve.
| Drug | Brand name | Main indication | Mechanism | First major approval |
|---|---|---|---|---|
| Fomivirsen | Vitravene | Cytomegalovirus retinitis in AIDS | Antisense inhibition of viral RNA | 1998, US; later withdrawn for commercial reasons |
| Mipomersen | Kynamro | Homozygous familial hypercholesterolemia | RNase H-mediated reduction of apoB-100 mRNA | 2013, US; later withdrawn |
| Eteplirsen | Exondys 51 | Duchenne muscular dystrophy amenable to exon 51 skipping | Splice modulation / exon skipping | 2016, US |
| Nusinersen | Spinraza | Spinal muscular atrophy | Splice switching of SMN2 pre-mRNA | 2016, US |
| Inotersen | Tegsedi | Polyneuropathy of hereditary transthyretin-mediated amyloidosis | RNase H-mediated reduction of transthyretin mRNA | 2018, US/EU |
| Volanesorsen | Waylivra | Familial chylomicronemia syndrome | RNase H-mediated reduction of apoC-III mRNA | 2019, EU |
| Golodirsen | Vyondys 53 | Duchenne muscular dystrophy amenable to exon 53 skipping | Splice modulation / exon skipping | 2019, US |
| Viltolarsen | Viltepso | Duchenne muscular dystrophy amenable to exon 53 skipping | Splice modulation / exon skipping | 2020, Japan/US |
| Casimersen | Amondys 45 | Duchenne muscular dystrophy amenable to exon 45 skipping | Splice modulation / exon skipping | 2021, US |
| Tofersen | Qalsody | Amyotrophic lateral sclerosis associated with SOD1 mutation | RNase H-mediated reduction of SOD1 mRNA | 2023, US; 2024, EU |
| Eplontersen | Wainua | Polyneuropathy of hereditary transthyretin-mediated amyloidosis in adults | GalNAc-conjugated RNase H-mediated reduction of transthyretin mRNA | 2023, US |
| Olezarsen | Tryngolza | Familial chylomicronemia syndrome in adults | GalNAc-conjugated RNase H-mediated reduction of apoC-III mRNA | 2024, US |
| Donidalorsen | Dawnzera | Prevention of hereditary angioedema attacks | GalNAc-conjugated RNase H-mediated reduction of prekallikrein mRNA | 2025, US |
The approved-drug landscape illustrates two trends. First, the earliest successes were often local or rare-disease applications where a strong genetic mechanism justified a high development burden. Second, newer drugs increasingly use targeted delivery, especially GalNAc conjugation for liver-expressed genes. This has made liver targets such as transthyretin, apolipoprotein C-III and prekallikrein especially attractive for ASO development.
Delivery and Tissue Targeting
Delivery remains one of the main constraints on antisense therapy. ASOs are large, charged molecules compared with small-molecule drugs, so they do not cross cell membranes freely and are not suitable for ordinary oral dosing. Currently approved ASOs are given by subcutaneous injection, intravenous infusion, intrathecal injection into the cerebrospinal fluid or intravitreal injection into the eye.
The liver is one of the easiest organs to target because hepatocytes naturally take up many oligonucleotides and because GalNAc conjugation provides an efficient receptor-mediated route into those cells. The central nervous system is harder to reach from the bloodstream because of the blood-brain barrier, so neurological ASOs such as nusinersen and tofersen are delivered intrathecally. Muscle, lung and many solid tumors remain more difficult targets, although new conjugates, nanoparticles, peptides and local-delivery strategies are active areas of research.
Antisense Therapy and Related RNA-Targeted Approaches
Antisense therapy is often compared with RNA interference, gene therapy and mRNA therapy. These approaches overlap in that they all deal with genetic information, but they act at different biological levels.
| Approach | Typical molecule | Main target | Main therapeutic effect |
|---|---|---|---|
| Antisense therapy | Single-stranded ASO | RNA or pre-mRNA | Destroys, redirects or blocks a target RNA |
| RNA interference | Double-stranded siRNA | mRNA | Uses RISC to cleave target mRNA |
| Gene therapy | DNA vector or editing system | Genome | Adds, replaces, silences or edits genetic information |
| mRNA therapy | Messenger RNA | Cellular translation machinery | Instructs cells to make a therapeutic or vaccine protein |
The distinction from gene therapy is especially important: an antisense drug does not alter a patient's DNA. Its effects are usually reversible and last only as long as enough drug remains in the relevant tissue. This is why ASOs generally require repeat dosing. Antisense therapy is therefore a major branch of RNA therapy, alongside RNA interference, mRNA vaccines and other RNA-based medicines.
A Brief History of Antisense Therapy
The concept of antisense therapy was introduced in 1978, when Paul Zamecnik and Mary Stephenson showed that a short synthetic oligonucleotide complementary to Rous sarcoma virus RNA could inhibit viral replication in cell culture. The idea was powerful, but unmodified oligonucleotides were rapidly degraded by nucleases, entered cells poorly and sometimes provoked unwanted immune responses.
Through the 1980s and 1990s, academic groups and companies such as Isis Pharmaceuticals, now Ionis Pharmaceuticals, developed chemical modifications that stabilized oligonucleotides without eliminating their biological activity. The first approved antisense drug, fomivirsen, was authorized by the FDA in 1998 for cytomegalovirus retinitis in patients with AIDS, but it was later withdrawn for commercial reasons after antiretroviral therapy sharply reduced the need for the drug.
The field's modern inflection point came in 2016 with the approval of nusinersen for spinal muscular atrophy. It showed that a splice-switching ASO delivered to the central nervous system could produce major clinical benefit in a severe genetic disease. Subsequent approvals for Duchenne muscular dystrophy, hereditary transthyretin-mediated amyloidosis, SOD1-ALS, familial chylomicronemia syndrome and hereditary angioedema have made antisense therapy one of the most established forms of RNA medicine.
Safety, Limitations, and Future Directions
The safety profile of an ASO depends on its sequence, chemistry, dose, tissue exposure and route of administration. Chemistry-related risks can include platelet effects, kidney effects, liver enzyme elevations, complement activation or innate immune stimulation. Sequence-related risks include unintended hybridization with partially matched RNAs. Route-related risks include lumbar puncture complications for intrathecal drugs and ocular procedure risks for intravitreal drugs. These concerns are managed through careful sequence screening, chemistry selection, dose optimization and clinical monitoring.
Despite these limitations, several ASOs have shown acceptable benefit–risk profiles in severe genetic diseases where few alternatives exist. The main scientific barriers are now delivery to difficult tissues, durable activity at lower doses, better prediction of off-target effects and expansion beyond rare diseases. The main practical barriers are cost, manufacturing scale and equitable access. Several approved ASOs for rare neuromuscular and neurodegenerative diseases carry prices in the hundreds of thousands of dollars per patient per year, which makes reimbursement and long-term access central parts of the clinical story.
A particularly striking direction is the development of individualized antisense drugs. In 2019, a team at Boston Children's Hospital reported the design, manufacture and administration of an ASO called milasen for a single child with an ultra-rare form of Batten disease. Such n-of-1 drugs raise scientific, regulatory and ethical questions that conventional drug development was not designed to answer, but they also show why antisense technology is attractive for rare sequence-defined disorders. A custom ASO can sometimes be designed more rapidly than a conventional small molecule or biologic, although safety testing remains essential.
Frequently Asked Questions
Is antisense therapy the same as gene therapy? No. Gene therapy alters or adds DNA in a patient's cells, or edits the genome directly. Antisense therapy works at the RNA level. It does not change the genome, so its effects usually require repeat dosing.
How is antisense therapy different from RNA interference? Both approaches target RNA, but they use different molecular machinery. Antisense oligonucleotides are single-stranded molecules that bind RNA directly and may recruit RNase H, alter splicing or block translation. RNA interference uses double-stranded small interfering RNAs that load into the RISC complex, which then finds and cleaves target mRNA.
What diseases are antisense therapies used for? Approved antisense therapies are used for selected rare and genetic diseases, including spinal muscular atrophy, Duchenne muscular dystrophy, SOD1-linked amyotrophic lateral sclerosis, hereditary transthyretin-mediated amyloidosis, familial chylomicronemia syndrome and prevention of hereditary angioedema attacks. Research programs are also exploring cancer, metabolic, cardiovascular, neurological and inflammatory diseases.
Are antisense drugs given as pills? Currently approved antisense oligonucleotides are not ordinary oral pills. They are degraded in the gut and absorbed poorly, so approved products are given by injection or infusion. Routes include subcutaneous injection, intravenous infusion, intrathecal injection into the spinal canal and intravitreal injection into the eye.
Can antisense therapy cure genetic diseases? In most cases, antisense therapy controls a disease rather than curing it. Because the underlying DNA remains unchanged, the abnormal RNA can continue to be produced. Treatment must usually be repeated to maintain the therapeutic effect.
Why are antisense drugs so expensive? Most approved ASOs treat rare or ultra-rare diseases, so development and manufacturing costs are spread across small patient populations. Chemically modified oligonucleotides are also more complex to manufacture than many small molecules. Prices and patient access vary widely by country, health system and indication.
Can antisense therapy be designed for a single patient? In rare circumstances, yes. Milasen, an individualized splice-switching ASO designed for one child with a unique form of Batten disease, is the best-known example. Such approaches remain exceptional and raise unresolved regulatory, ethical and safety questions, but they demonstrate the programmability of the antisense platform.
Further Reading
Nature Reviews Drug Discovery, Antisense Technology: An Overview and Prospectus
Nucleic Acids Research, Chemistry, Structure and Function of Approved Oligonucleotide Therapeutics
BioDrugs, Mechanisms of Action of the US Food and Drug Administration-Approved Antisense Oligonucleotide Drugs
New England Journal of Medicine, Trial of Antisense Oligonucleotide Tofersen for SOD1 ALS
New England Journal of Medicine, Olezarsen, Acute Pancreatitis, and Familial Chylomicronemia Syndrome