RNA Therapy: Types, Mechanisms, Delivery and Approved Uses
What Is RNA Therapy?
Plain-language definition: RNA therapy is medicine that works by adding, blocking, or changing RNA instructions inside cells. More formally, it is a class of treatment that uses RNA molecules, or drugs that act on RNA, to change which proteins a cell makes – either silencing a harmful protein, correcting how a gene is read, or instructing cells to produce a needed protein.
RNA therapy, also called RNA therapeutics, is a family of medicines built from or directed against RNA, the molecule that normally carries instructions from a cell's DNA to its protein-making machinery. Rather than blocking a finished protein the way most conventional drugs do, RNA therapies act one step earlier, at the level of the genetic message itself. Depending on the design, an RNA drug can switch off the production of a disease-causing protein, redirect how a gene's message is assembled, or supply a working message so the cell manufactures a protein it cannot make on its own.
This approach widens the range of treatable targets considerably. Small-molecule drugs generally need a protein with a well-defined pocket to bind, and biologic drugs such as antibodies mostly act on proteins outside the cell. Because RNA therapies recognize their target through simple nucleic acid base pairing, they can in principle be aimed at almost any gene message, including those that produce so-called undruggable proteins. The field moved from concept to clinic over roughly two decades: the first antisense drug was approved in 1998, and by the mid-2020s more than two dozen RNA or oligonucleotide-based medicines had received FDA and/or EMA approval, alongside the mRNA vaccines deployed against COVID-19.
At a glance:
- What it is: medicines made from, or directed against, RNA
- Core principle: targeting works by nucleic acid base pairing
- Main effects: silence a protein, correct splicing, or supply a protein
- Main modalities: antisense oligonucleotides, siRNA, mRNA, aptamers
- Key advantage: can address targets unreachable by small molecules
- Central challenge: delivering RNA into the right cells
How Does RNA Therapy Work?
All RNA therapies exploit the same recognition principle: a designed strand of nucleic acid finds its target by complementary base pairing, the same rule that lets the two strands of DNA zip together. From that shared starting point, different modalities produce very different outcomes. The cleanest way to understand the field is to group these outcomes into three jobs: shutting a message down, rewriting how a message is read, and adding a message that was missing.
The first job is gene silencing. A short small interfering RNA (siRNA) is loaded into a natural cellular machine and uses one of its strands as a guide to find the matching messenger RNA, which is then cut and destroyed. This co-opts RNA interference, a defensive pathway cells use against double-stranded RNA. A single-stranded gapmer antisense oligonucleotide can achieve a similar result by a different route: when it pairs with its target message, an enzyme called RNase H recognizes the RNA–DNA hybrid and degrades the message, lowering the amount of the corresponding protein.
The second job is correcting how a gene's message is processed. Before a message is used, non-coding stretches are removed and the remaining pieces are joined in a step called splicing. A carefully placed oligonucleotide can mask a splicing signal so the cell includes or skips a particular segment, producing a more functional protein from a faulty gene. This splice-switching strategy underlies the spinal muscular atrophy drug nusinersen, which restores production of a needed protein without destroying any message.
The third job is supplying a message the body needs. A synthetic messenger RNA, read by the ribosome like any natural transcript, instructs cells to manufacture a chosen protein for as long as the message survives. The same logic powers mRNA vaccines, where the encoded protein is a pathogen antigen, and is being extended to deliver therapeutic proteins directly. A fourth, increasingly important role is to act as a guide: in CRISPR systems an engineered guide RNA directs a DNA-cutting enzyme to a precise genomic site, making RNA the targeting component of gene editing as well.
The Main Types of RNA Therapeutics
Although they share a recognition principle, RNA modalities differ in chemistry, mechanism and the kind of disease they suit. Most RNA drugs are not simply unmodified natural RNA; they use chemical changes to improve stability, reduce immune sensing and tune how long the drug acts. Antisense oligonucleotides and siRNAs lower the level of a target protein and are well matched to conditions caused by a toxic or overexpressed protein. Messenger RNA does the opposite, restoring a protein that is absent or insufficient, and is also the basis of vaccines. Aptamers work differently again: they fold into shapes that bind and block a target protein much like an antibody. The table below summarizes the principal classes and how they act.
| Term | Meaning |
|---|---|
| RNA therapy | Umbrella term for medicines made from RNA or designed to act on RNA messages |
| RNA interference (RNAi) | Natural gene-silencing pathway used by siRNA drugs |
| mRNA therapy | RNA therapy that adds a message for cells to translate into a protein or antigen |
| Antisense therapy | Oligonucleotide therapy that binds RNA to degrade a message or change how it is spliced |
| RNA modality | Mechanism of action | Therapeutic effect | Representative approved drug |
|---|---|---|---|
| Antisense oligonucleotide (ASO) | Single strand base-pairs with a target message; triggers its degradation or alters its splicing | Reduces a harmful protein or corrects a defective one | Nusinersen (spinal muscular atrophy) |
| Small interfering RNA (siRNA) | Double strand loaded into the RNA interference machinery; guides cleavage of the matching message | Durably silences a disease-causing protein | Patisiran (hereditary transthyretin amyloidosis) |
| Messenger RNA (mRNA) | Synthetic message translated by ribosomes into a chosen protein or antigen | Supplies a missing protein or trains the immune system | COVID-19 mRNA vaccines |
| Aptamer | Folded RNA or other nucleic-acid aptamer binds a target protein by shape, blocking its function | Inhibits a protein much like an antibody | Pegaptanib (neovascular eye disease) |
A non-obvious trade-off runs through this comparison. The silencing modalities are extremely durable once delivered, so a single dose can suppress a target for weeks to months, but their reach is limited mainly to tissues that current delivery tools can access. Messenger RNA can address an enormous range of proteins, yet its effect is comparatively short-lived because the message is consumed and degraded, which is well suited to vaccination but more demanding for chronic protein replacement. Related approaches such as microRNA mimics and inhibitors and small activating RNAs that raise rather than lower gene expression broaden the toolkit further but are mostly still in development.
Approved RNA Therapies and Clinical Use
The clinical record of RNA therapy began in 1998 with fomivirsen, an antisense drug for a viral eye infection, followed in 2004 by pegaptanib, the first aptamer drug, for neovascular age-related macular degeneration. The field's modern era opened in 2016 with nusinersen for spinal muscular atrophy, a splice-switching oligonucleotide that markedly changed the course of a previously fatal infant disease, and in 2018 with patisiran, the first siRNA drug, which silences the transthyretin message to treat hereditary transthyretin amyloidosis using a lipid-nanoparticle delivery system.
Since then, approved RNA medicines have expanded across several modalities. Antisense oligonucleotides include eteplirsen and related exon-skipping drugs for Duchenne muscular dystrophy and tofersen for a genetic form of amyotrophic lateral sclerosis. Approved siRNA examples include givosiran for acute hepatic porphyria, lumasiran and nedosiran for primary hyperoxaluria, vutrisiran for transthyretin amyloidosis and inclisiran for cholesterol lowering. Inclisiran is notable because it silences PCSK9 and is dosed only about twice a year, extending RNA therapy from rare genetic conditions toward a common cardiovascular indication. These medicines have become part of the broader landscape of biopharmaceuticals.
| Representative drug or product | Modality | Target disease or use | Delivery route or strategy |
|---|---|---|---|
| Nusinersen | Splice-switching ASO | Spinal muscular atrophy | Injection into spinal fluid |
| Patisiran | siRNA | Hereditary transthyretin amyloidosis | Lipid nanoparticle |
| Givosiran | siRNA | Acute hepatic porphyria | GalNAc conjugate |
| Inclisiran | siRNA | LDL cholesterol lowering through PCSK9 silencing | GalNAc conjugate |
| Tofersen | ASO | SOD1-linked amyotrophic lateral sclerosis | Injection into spinal fluid |
| COVID-19 mRNA vaccines | mRNA | Infectious-disease vaccination | Lipid nanoparticle |
| Pegaptanib | Aptamer | Neovascular eye disease | Injection into the eye |
The most visible medical use of RNA technology is the messenger RNA vaccine. The COVID-19 mRNA vaccines developed by Pfizer–BioNTech and Moderna delivered, at unprecedented scale, a lipid-encapsulated message encoding the viral spike protein, validating the platform and accelerating investment across the field. Because an mRNA drug can encode essentially any protein, it can be redesigned quickly. The same technology is now being applied to individualized cancer vaccines and to in-body production of therapeutic proteins, both closely tied to the goals of personalized medicine.
Delivery: The Central Challenge of RNA Therapy
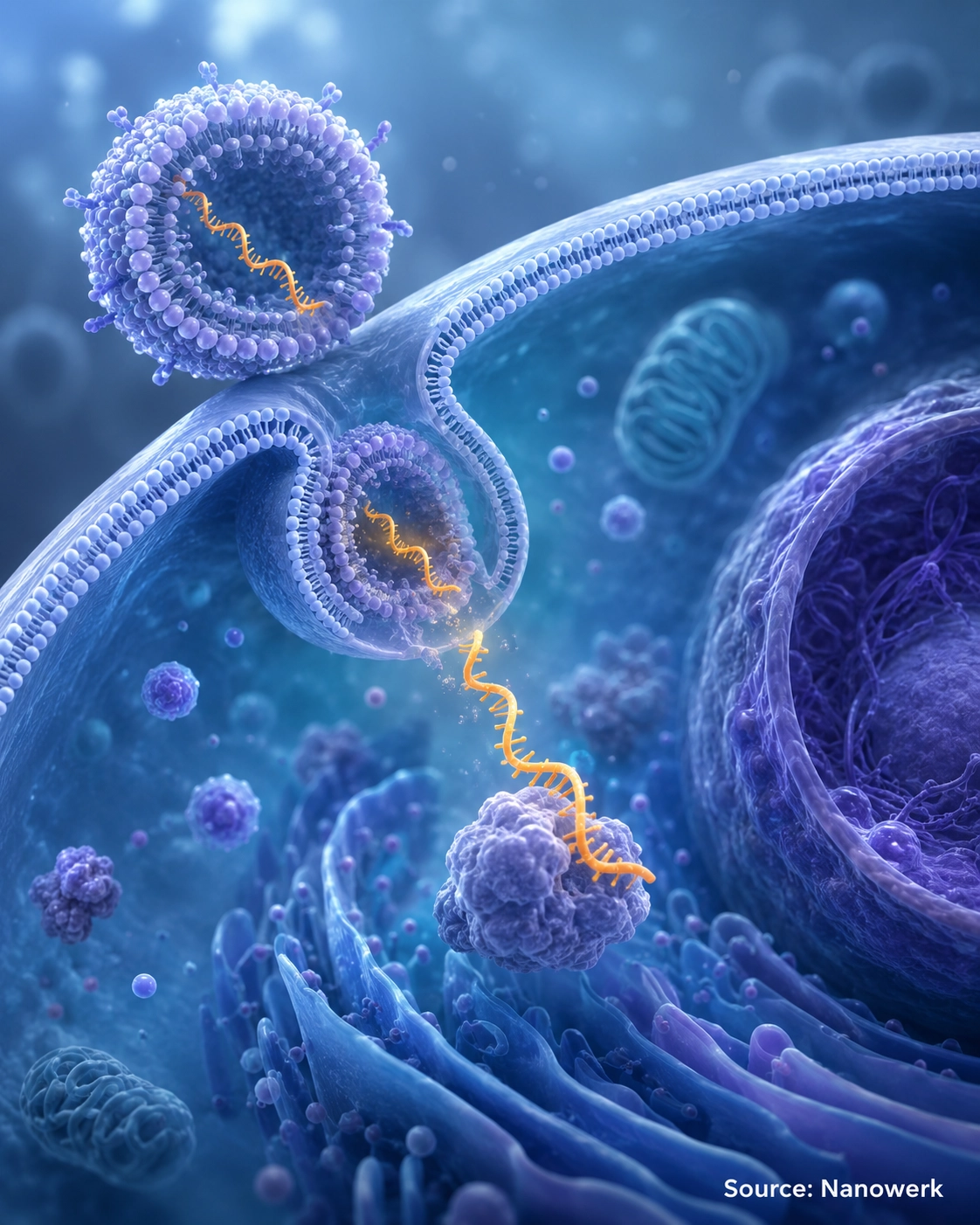
RNA is a difficult drug to deliver. It is large, negatively charged and cannot cross cell membranes on its own, and unprotected RNA is rapidly chopped up by nucleases in blood and tissue. Naked oligonucleotides are also filtered quickly by the kidney. Solving these problems has required as much engineering as the RNA sequence itself, and progress in delivery, more than in target selection, has paced the field.
Two strategies dominate the approved drugs. Lipid nanoparticles wrap the RNA in a protective fatty shell that shields it, helps it enter cells and tends to accumulate in the liver; this is the system used by patisiran and by the mRNA vaccines. The second strategy attaches a sugar tag called GalNAc to the RNA, which binds a receptor found almost exclusively on liver cells and pulls the drug into them with high specificity. Heavy chemical modification of the RNA backbone and sugars complements both approaches, dramatically increasing stability and reducing unwanted immune activation.
The consequence is that many approved systemic RNA-silencing drugs act on the liver, because that is the organ current delivery tools reach efficiently. Extending RNA therapy to muscle, the central nervous system, the lung, the kidney and tumors is the dominant problem in the field. Local administration partly sidesteps it: nusinersen is injected into spinal fluid and several aptamers are delivered directly into the eye, both routes that place the drug where it is needed and avoid the systemic delivery barrier entirely.
Is RNA Therapy Safe?
RNA drugs raise a distinct safety profile rather than an inherently better or worse one. Because synthetic RNA can resemble the molecular patterns of a viral infection, an unmodified sequence may trigger an unwanted innate immune response. The goal is not to make RNA invisible in every context: vaccines deliberately use delivery and formulation to generate immunity, whereas protein-replacement or silencing therapies usually try to minimize inflammatory sensing. The standard solution is chemical modification, including substitutions in the sugar-phosphate backbone and the use of modified bases; incorporating a modified version of one nucleotide was a key step in making mRNA vaccines tolerable and effective.
Two other risks shape design. An RNA drug may partially match unintended messages and silence the wrong gene, an off-target effect minimized through careful sequence selection and computational screening. Delivery vehicles carry their own liabilities, including infusion reactions and effects on the liver where most drugs concentrate, which is why some regimens use premedication. A practical limitation rather than a safety issue is that, because RNA and its effects eventually decay, most therapies must be redosed periodically, and several oligonucleotide drugs for ultra-rare diseases have launched at very high prices, raising real questions about access.
Future Perspectives
The near-term trajectory of RNA therapy is defined less by new mechanisms than by escaping the liver. Conjugate chemistries and nanoparticle designs aimed at muscle, the nervous system and the lung are advancing through trials, and success there would multiply the number of treatable diseases. In parallel, RNA is becoming the targeting and editing component of genome medicine: chemically synthesized guide RNAs direct CRISPR systems, and message-level RNA editing using the cell's own ADAR enzymes offers a way to make precise, reversible changes without cutting DNA, complementing approaches such as base editing and prime editing.
Newer formats are maturing as well. Self-amplifying RNA copies itself briefly inside the cell, promising similar effects at much lower doses, and circular RNA is engineered for greater stability and longer protein output. Together with individualized cancer vaccines, these directions point toward RNA therapy moving beyond rare genetic disease into common conditions. As a programmable, sequence-defined modality, RNA therapeutics have become one of the fastest-moving areas of modern biotechnology, with the central question now being how broadly and how safely they can be delivered.
Frequently Asked Questions
What is the difference between RNA therapy and gene therapy? Classical gene therapy delivers a permanent DNA copy of a gene that integrates into or persists in the cell and is meant to provide a lasting correction. RNA therapy instead delivers or targets RNA, so its effect is transient and dose-dependent and does not change the genome. This makes RNA therapy more reversible and easier to titrate, but it usually requires repeat dosing because the RNA and its effect eventually decay.
Are mRNA vaccines a form of RNA therapy? Yes. mRNA vaccines are the most widely deployed medical use of messenger RNA technology. They deliver a synthetic mRNA that instructs cells to make a target protein, in this case a pathogen antigen, so the immune system learns to recognize it. The same messenger RNA platform is being developed to supply therapeutic proteins and personalized cancer vaccines.
Why do many systemic RNA-silencing drugs target the liver? Delivery is the central obstacle for RNA drugs, and the liver is one of the easiest organs to reach from the bloodstream. Lipid nanoparticles tend to accumulate in the liver, and sugar tags called GalNAc bind a receptor found almost exclusively on liver cells. Many approved systemic RNA-silencing drugs use one of these two strategies, which is why they target proteins made in the liver. Reaching other tissues efficiently remains an active research problem.
Is RNA therapy permanent? Generally no. Because RNA and its effects are eventually broken down, most RNA therapies require periodic redosing, ranging from every few weeks to roughly twice a year depending on the drug and chemistry. The exception is when RNA is used only as a temporary guide for a gene-editing system, where the RNA disappears but the DNA edit it directed is permanent.
What diseases can RNA therapy treat? Approved RNA therapies treat spinal muscular atrophy, hereditary transthyretin amyloidosis, acute hepatic porphyria, certain high-cholesterol conditions, Duchenne muscular dystrophy and several other rare genetic diseases, and mRNA vaccines protect against infectious disease. Many additional candidates are in clinical trials for cancer, cardiovascular and neurological conditions.
Further Reading
Nature Reviews Drug Discovery, Frameworks for Transformational Breakthroughs in RNA-Based Medicines
Nature Reviews Drug Discovery, RNAi-Based Drug Design: Considerations and Future Directions
Nature Reviews Drug Discovery, Tailor Made: The Art of Therapeutic mRNA Design
Nature Reviews Drug Discovery, Amplifying Gene Expression with RNA-Targeted Therapeutics
Nature Reviews Drug Discovery, RNA Chemistry and Therapeutics
