Signal Transduction: Pathways, Mechanisms, and Therapeutic Targets
What Is Signal Transduction?
Signal transduction The cellular process that converts a signal, such as a hormone, growth factor, neurotransmitter, cytokine, mechanical force, or environmental cue, into biochemical changes inside the cell that alter behavior, gene expression, metabolism, movement, survival, or division.
Signal transduction is a core part of cell signaling, the broader field that studies how cells send, receive, process, and respond to information. In a typical pathway, a signal binds a receptor at the cell surface or inside the cell, that receptor activates a relay of intracellular molecules, and the relay produces a defined biological response. This conversion of an external cue into an internal decision allows cells to coordinate development, immunity, metabolism, tissue repair, neuronal communication, and programmed cell death.
In simple terms, signal transduction is how cells translate “what is happening outside” into “what to do about it.” The classic sequence is reception, transduction, and response. Reception detects the cue; transduction amplifies and routes the information; response changes the cell. The same basic logic appears across eukaryotic life, but mammalian cells use especially dense signaling networks because they must integrate hormones, growth factors, nutrients, mechanical signals, pathogens, neighboring cells, and stress cues at the same time.
Modern biology treats signal transduction as a network rather than a set of isolated linear pipelines. A mammalian cell may express hundreds of receptors and route information through dozens of overlapping pathways, with feedback loops, crosstalk, scaffold proteins, compartment-specific signaling, and tissue-specific tuning. This network logic explains why the same signaling molecule can trigger proliferation in one cell type, differentiation in another, and death or immune activation in a third.
Signaling components are also central drug targets. GPCRs are targeted by roughly one-third of approved medicines, and by late 2025 the FDA had approved about 100 small-molecule kinase inhibitors, most for oncology and a growing number for inflammatory or immune-mediated disease. Dysregulated signaling underlies cancer, type 2 diabetes, autoimmune disease, cardiovascular disease, and many neurological disorders, making the field a central pillar of modern biotechnology.
Synonyms: cell signaling, cellular signaling, signaling cascade, signaling pathway (when referring to a specific route).
Not to be confused with: gene regulation, which is one common endpoint of signal transduction rather than a synonym for it. A signaling pathway can also produce non-transcriptional outputs such as ion-channel opening, cytoskeletal rearrangement, secretion, or metabolic change.
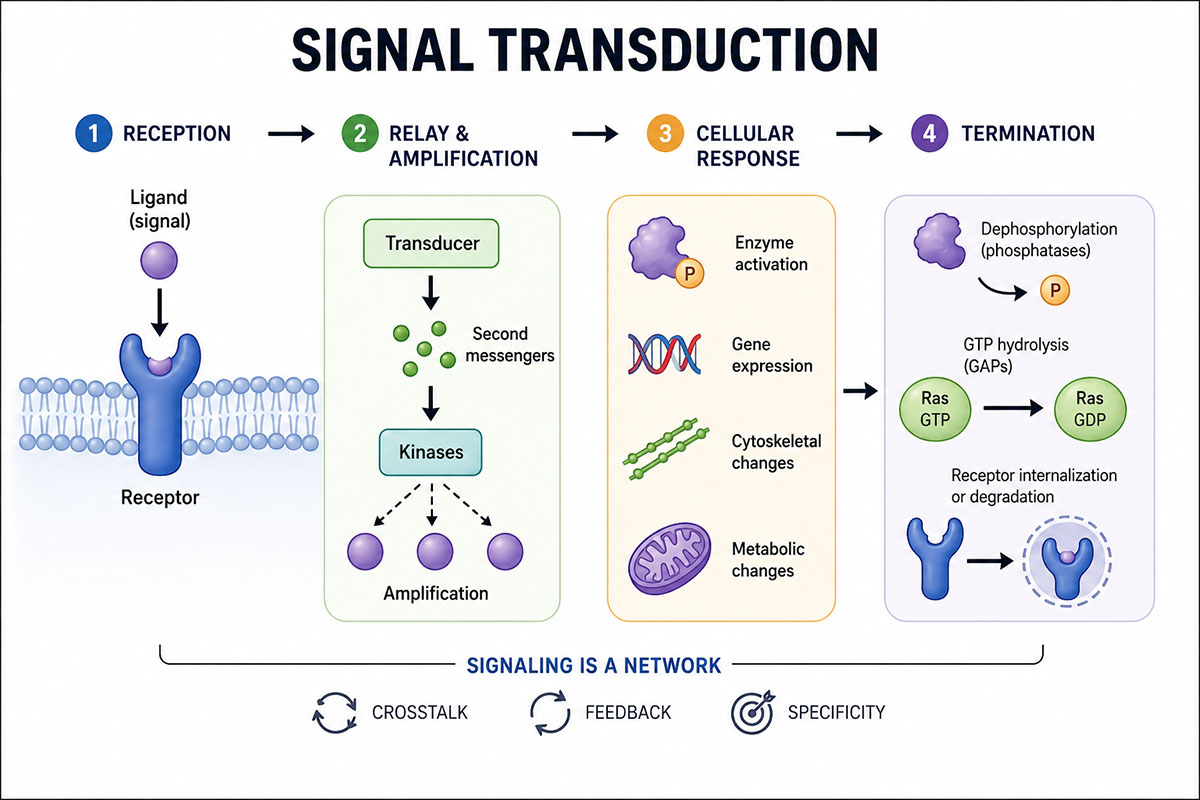
Signal transduction in simplified form: a signal binds a receptor, the activated receptor relays and amplifies the message inside the cell, and the cell produces a response. Signaling pathways are regulated by feedback and shutdown mechanisms that keep the response controlled. (Image: Nanowerk) (click on image to enlarge)
Key Components of a Signaling Pathway
| Component | Role in signal transduction | Examples |
|---|---|---|
| Ligand or first messenger | External or environmental cue that initiates signaling | Insulin, epidermal growth factor, adrenaline, cytokines, neurotransmitters |
| Receptor | Detects the signal and converts binding into a biochemical change | Receptor tyrosine kinases, GPCRs, cytokine receptors, ion channels, nuclear receptors |
| Transducer | Relays the signal inside the cell through enzymatic activity or protein-protein interactions | G proteins, kinases, adaptor proteins, scaffold proteins |
| Second messenger | Small intracellular molecule that rapidly amplifies or distributes the signal | cAMP, cGMP, Ca2+, IP3, DAG, PIP3 |
| Effector | Executes the response by changing enzyme activity, ion flow, cytoskeletal behavior, secretion, or transcription | Protein kinases, ion channels, metabolic enzymes, transcription factors |
| Feedback regulator | Tunes, limits, or terminates the pathway | Phosphatases, GTPase-activating proteins, receptor internalization, SOCS proteins |
Major Receptor Classes
Receptors determine which signals a cell can detect. Some sit in the plasma membrane and sense ligands outside the cell; others are intracellular and respond to molecules that cross the membrane, such as steroid hormones. The most important receptor classes in mammalian signal transduction include receptor tyrosine kinases, G protein-coupled receptors, cytokine receptors, ligand-gated ion channels, integrins, pattern-recognition receptors, and intracellular nuclear receptors.
| Receptor class | Typical signal | Common signaling output |
|---|---|---|
| Receptor tyrosine kinases (RTKs) | Growth factors such as EGF, VEGF, insulin, and PDGF | MAPK and PI3K/AKT activation, growth, survival, metabolism |
| G protein-coupled receptors (GPCRs) | Hormones, neurotransmitters, chemokines, odors, light | cAMP, calcium, IP3/DAG, ion-channel regulation |
| Cytokine receptors | Interferons, interleukins, colony-stimulating factors | JAK-STAT signaling, immune activation, hematopoiesis |
| Ligand-gated ion channels | Neurotransmitters such as glutamate, GABA, acetylcholine | Rapid ion flux and electrical signaling |
| Integrins and adhesion receptors | Extracellular matrix proteins and cell-adhesion cues | Cytoskeletal remodeling, survival, migration, mechanotransduction |
| Nuclear receptors | Steroid hormones, thyroid hormone, retinoids, vitamin D | Direct regulation of gene transcription |
How Signal Transduction Works
1. Reception
Reception begins when a ligand binds its receptor with appropriate specificity and affinity. Receptor tyrosine kinases dimerize and phosphorylate one another. GPCRs activate heterotrimeric G proteins. Cytokine receptors recruit JAK kinases. Ligand-gated ion channels open pores in the membrane within milliseconds. Intracellular nuclear receptors bind membrane-permeable ligands and act directly as transcriptional regulators.
2. Relay and amplification
Transduction begins once the receptor is activated. The dominant chemical move in mammalian signaling is reversible protein phosphorylation: a kinase adds a phosphate group to serine, threonine, or tyrosine residues, and a phosphatase removes it. Edmond Fischer and Edwin Krebs received the 1992 Nobel Prize in Physiology or Medicine for establishing this principle in the 1950s. The human kinome, the complete set of human protein kinases, comprises 518 members, many organized into hierarchical cascades. In most mammalian protein kinase reactions, phosphorylation consumes ATP and changes the substrate’s shape, charge, location, or binding partners.
Amplification is what makes signal transduction powerful. One activated receptor can activate many G proteins, one kinase can phosphorylate many substrates, and one enzyme can generate thousands of second-messenger molecules. Earl Sutherland coined the term second messenger after discovering cyclic AMP, work that earned the 1971 Nobel Prize. The major second messengers include cyclic AMP, cyclic GMP, calcium ions, inositol trisphosphate, diacylglycerol, and the membrane lipid PIP3. This amplification allows very low concentrations of hormones or growth factors to produce large cellular effects.
3. Cellular response
The response stage is where signaling becomes a decision. Some responses are immediate, such as ion-channel opening, secretion, muscle contraction, cytoskeletal remodeling, or metabolic enzyme activation. Others are slower because they require transcription factors to enter the nucleus and change gene transcription. STAT proteins, NF-κB, SMAD proteins, FOXO factors, and the AP-1 complex are common transcriptional endpoints.
Cells do not simply read signaling pathways as on or off. They interpret signal strength, duration, timing, pulse frequency, and location. A brief ERK pulse can produce a different outcome than sustained ERK activation; calcium oscillation frequency can encode stimulus intensity; and NF-κB dynamics help shape inflammatory gene expression. Spatial organization also matters: receptors can continue signaling from endosomes, kinases may be confined by scaffold proteins, and lipid rafts, organelles, and biomolecular condensates can concentrate pathway components in specific parts of the cell.
4. Termination and reset
Signaling must be reversible. Cells switch pathways off through phosphatases, receptor desensitization, receptor internalization and degradation, GTP hydrolysis by G proteins and small GTPases, second-messenger breakdown, and transcription of feedback inhibitors. These brakes prevent transient cues from locking a cell into a permanent state. They also create adaptation, allowing a cell to respond to a new change in stimulus rather than remain saturated by the previous one.
Major Signal Transduction Pathways
Most clinically important signaling in mammalian cells routes through a set of well-characterized pathways. MAPK, PI3K/AKT/mTOR, JAK-STAT, and GPCR signaling account for much of current pharmacology, while Wnt, Hedgehog, Notch, TGF-β/SMAD, NF-κB, and Hippo signaling are central to development, immunity, regeneration, inflammation, and cancer biology.
| Pathway | Initiating receptor | Key effectors | Major outputs | Drug examples |
|---|---|---|---|---|
| MAPK (RAS/RAF/MEK/ERK) | Receptor tyrosine kinases such as EGFR and HER2 | RAS, RAF, MEK1/2, ERK1/2 | Proliferation, differentiation, survival | BRAF inhibitors such as vemurafenib and dabrafenib; MEK inhibitors such as trametinib |
| PI3K/AKT/mTOR | RTKs, GPCRs, integrins | PI3K, PTEN, AKT, mTORC1, mTORC2 | Cell growth, metabolism, survival, autophagy | PI3K inhibitors such as alpelisib; AKT inhibitors such as capivasertib; mTOR inhibitors such as everolimus |
| JAK-STAT | Type I and type II cytokine receptors | JAK1, JAK2, JAK3, TYK2; STAT1–6 | Immune response, hematopoiesis, inflammation | JAK inhibitors such as tofacitinib, ruxolitinib, and baricitinib |
| GPCR / heterotrimeric G protein | Approximately 800 G protein-coupled receptors | Gαs, Gαi, Gαq; cAMP, IP3, DAG; β-arrestin | Hormone responses, neurotransmission, sensory perception, immune trafficking | Beta-blockers, antihistamines, opioids, antipsychotics, GLP-1 receptor agonists |
| Additional pathway | Why it matters | Typical biological role |
|---|---|---|
| Wnt/β-catenin | Controls cell fate and is frequently altered in colorectal cancer | Development, stem-cell maintenance, tissue renewal |
| Notch | Uses direct cell-cell contact to regulate fate decisions | Development, immune differentiation, vascular biology |
| Hedgehog | Patterning pathway reactivated in some cancers | Embryonic development, tissue patterning, repair |
| TGF-β/SMAD | Can suppress early tumors but promote invasion and fibrosis later | Cell-cycle control, immune regulation, extracellular matrix remodeling |
| NF-κB | Central inflammatory and stress-response pathway | Innate immunity, cytokine production, survival under stress |
| Hippo/YAP-TAZ | Links organ size, mechanics, and growth control | Regeneration, mechanotransduction, proliferation |
Pathways do not operate independently. Crosstalk, such as ERK feedback inhibition of upstream RTK signaling or PI3K activation downstream of GPCRs, means that real cells integrate multiple inputs simultaneously. This is why drugs targeting one pathway can trigger compensatory activation in another. The same kinases that drive proliferation in cancer also coordinate normal embryonic development, immune activation, wound repair, and metabolic adaptation, so therapeutic targeting must balance efficacy with toxicity.
Signal Transduction in Disease
Cancer is the clearest example of what happens when signal transduction goes wrong. RAS-family mutations occur in roughly one-fifth of cancer patients overall. KRAS mutations are especially common in pancreatic adenocarcinoma and occur in substantial subsets of colorectal cancer and lung adenocarcinoma. BRAF V600E mutations drive a large fraction of cutaneous melanomas, and PIK3CA mutations are among the most common alterations in breast and gynecological cancers. These mutations lock signaling nodes in an “on” state or remove them from normal feedback control. Receptor tyrosine kinases are similarly affected: HER2 amplification in breast cancer, EGFR mutations in lung adenocarcinoma, and BCR-ABL fusions in chronic myelogenous leukemia all create constitutively active signaling that drives proliferation independent of upstream cues.
Beyond oncology, dysregulated signal transduction underlies a broad range of human disease. JAK-STAT mutations cause primary immunodeficiencies and contribute to rheumatoid arthritis, psoriasis, myeloproliferative neoplasms, and inflammatory bowel disease. Defects in insulin receptor and PI3K/AKT signaling are central to insulin resistance and type 2 diabetes. Abnormal GPCR signaling is important in heart failure, asthma, migraine, depression, psychosis, pain, and endocrine disease. In neurodegeneration, signaling defects are more distributed but include disrupted calcium signaling, impaired neurotrophin signaling, chronic inflammatory NF-κB and JAK-STAT activity, and altered insulin/PI3K-AKT signaling in Alzheimer’s disease research.
Identifying which signaling pathway is dysregulated in a given patient has become central to personalized medicine. Tumor sequencing, phosphoproteomic profiling, circulating biomarkers, and pathway-specific companion diagnostics can reveal whether a disease is driven by EGFR, ALK, HER2, BRAF, JAK, PI3K, or another actionable signaling node. The affected pathway often provides the most rational therapeutic target.
Targeted Therapies and Drug Development
The therapeutic exploitation of signal transduction became a defining feature of modern medicine with targeted cancer therapy. Trastuzumab (Herceptin), a monoclonal antibody against HER2, was approved in 1998 for HER2-positive breast cancer and established the biologics paradigm for blocking receptor signaling at the cell surface. Imatinib (Gleevec), approved in 2001 for chronic myelogenous leukemia, inhibited the BCR-ABL tyrosine kinase produced by the Philadelphia chromosome and helped turn a once-fatal leukemia into a chronic disease for many patients.
By late 2025, the FDA had approved about 100 small-molecule kinase inhibitors, most for oncology and an increasing number for inflammatory, immune-mediated, and rare diseases. GPCRs remain one of the largest drug-target families, with roughly one-third of approved medicines acting through GPCR targets. Antibodies against receptors and circulating ligands are another major class, including drugs that block HER2, EGFR, VEGF, TNF, IL-6, IL-17, IL-23, and immune checkpoints. Together, signaling-targeted small molecules and biopharmaceuticals form the backbone of targeted therapy in oncology, immunology, metabolic disease, cardiovascular medicine, and neuroscience.
Resistance is the recurring problem. Tumors treated with a single kinase inhibitor may reactivate the inhibited pathway, mutate the drug-binding site, amplify the target, switch to a bypass pathway, or rely on signals from the tumor microenvironment. Examples include MAPK reactivation after RAF or MEK inhibition, EGFR resistance mutations after EGFR inhibitor therapy, and PI3K pathway compensation after upstream blockade. Combination regimens, next-generation inhibitors, allosteric modulators, covalent inhibitors, PROTAC degraders, bispecific antibodies, antibody-drug conjugates, and biomarker-guided patient selection are major responses to this challenge.
How Researchers Study Signal Transduction
Most signal-transduction biology is still read out through phosphorylation. Phospho-specific antibodies that recognize a particular phosphorylated residue, such as phospho-ERK Thr202/Tyr204 or phospho-AKT Ser473, are standard tools in Western blot, immunofluorescence, flow cytometry, and ELISA assays. These methods ask whether a pathway is active in a particular cell type, tissue, or patient sample.
Phospho-proteomics extends this readout to thousands of phosphorylation sites in parallel using high-resolution mass spectrometry and phosphopeptide enrichment. Genetic perturbation has reshaped the discipline as well: CRISPR-Cas9 knockouts, CRISPR interference, CRISPR activation, RNA interference, and base-editing screens can map dependencies and resistance mechanisms across pathway components. Live-cell imaging with fluorescent biosensors now allows researchers to watch ERK, PKA, calcium, Rho GTPases, and other signaling activities move through single cells in real time.
Single-cell technologies are making pathway analysis more precise. Single-cell RNA sequencing reveals transcriptional outputs, spatial transcriptomics maps responses within tissue architecture, and multiplexed imaging can measure many signaling markers in the same tissue section. These approaches show that average pathway activity can hide major cell-to-cell differences, including rare drug-resistant states and immune-cell subsets that determine treatment response.
Frequently Asked Questions
What is the difference between a first messenger and a second messenger? A first messenger is the extracellular signal itself – a hormone, growth factor, neurotransmitter, cytokine, odorant, or other cue that binds a receptor on or inside the cell. A second messenger is a small intracellular molecule generated in response to receptor activation that propagates and amplifies the signal within the cell. Classic examples include cyclic AMP, calcium ions, inositol trisphosphate, diacylglycerol, and PIP3.
How is a signal transduction pathway switched off? Signaling responses are time-limited because cells deploy several termination mechanisms in parallel. Phosphatases remove activating phosphate groups added by kinases, GTPase-activating proteins return G proteins and small GTPases to their inactive GDP-bound state, second messengers are degraded or pumped back into stores, and receptor internalization removes activated receptors from the cell surface. Many pathways also induce feedback inhibitors such as SOCS proteins in JAK-STAT signaling.
What is a kinase cascade in signal transduction? A kinase cascade is a series of protein kinases that activate one another in sequence by phosphorylation, with each step amplifying and relaying the signal toward the cell’s response machinery. The MAPK pathway is the textbook example: activation of RAS recruits RAF, RAF phosphorylates MEK, MEK phosphorylates ERK, and ERK phosphorylates many substrates that change cellular behavior.
How fast does signal transduction happen? Speed varies by pathway and output. Ion channels can open within milliseconds of ligand binding, second-messenger responses such as calcium spikes or cyclic AMP bursts occur within seconds, and kinase cascades often peak within minutes. Transcriptional responses are slower, taking tens of minutes to hours, because they require changes in gene expression and protein production.
Why are signal transduction pathways important drug targets? Signaling pathways contain many druggable components, including receptors, kinases, phosphatases, ion channels, ligands, and downstream enzymes. GPCRs are targeted by roughly one-third of approved medicines, and by late 2025 the FDA had approved about 100 small-molecule kinase inhibitors. Antibody therapies against receptors and circulating ligands form another major category. Drugs that modulate signal transduction are central to targeted therapy in oncology, immunology, metabolic disease, cardiovascular medicine, and neuroscience.
Further Reading
Nature Reviews Drug Discovery, FDA Approves 100th Small-Molecule Kinase Inhibitor
Pharmacological Research, Properties of FDA-Approved Small Molecule Protein Kinase Inhibitors: A 2024 Update
Signal Transduction and Targeted Therapy, Targeting the RAS/RAF/MAPK Pathway for Cancer Therapy: From Mechanism to Clinical Studies
Signal Transduction and Targeted Therapy, Evolving Cognition of the JAK-STAT Signaling Pathway: Autoimmune Disorders and Cancer
Signal Transduction and Targeted Therapy, G Protein-Coupled Receptors (GPCRs): Advances in Structures, Mechanisms and Drug Discovery
