Drug Delivery: Definition, Methods, Nanocarriers, and Applications
What Is Drug Delivery?
In one sentence: Drug delivery is the engineering discipline concerned with controlling how, where, and when a therapeutic agent reaches its target in the body, so that it acts effectively while causing as little harm as possible to healthy tissue.
In simple terms: drug delivery is about getting the right amount of a medicine to the right place at the right time.
A drug molecule that works in a test tube is not yet a medicine. To be useful, it has to dissolve, survive the digestive tract or bloodstream, avoid premature breakdown, cross one or more biological barriers, accumulate where it is needed, and release its activity at a rate the body can use.
The conventional approach — swallowing a pill or injecting an unprotected drug molecule — leaves many of these steps to chance. Drug delivery takes deliberate control of them through formulations, carriers, implants, devices, and chemical modifications that govern the journey of the active compound from administration to its molecular site of action.
The need is large. Many promising drug candidates have poor water solubility or poor bioavailability, meaning that only a limited fraction of the administered dose reaches systemic circulation or the relevant tissue in active form. Conventional dosing also produces a characteristic peak-and-trough concentration curve: a spike shortly after each dose, often high enough to cause side effects, followed by a decline below the therapeutic threshold before the next dose. A well-designed delivery system flattens this curve, protects fragile cargo such as proteins and nucleic acids, and can concentrate the drug at the disease site, which is why drug delivery is one of the foundational application areas of nanomedicine and modern biopharmaceuticals.
Core functions of drug delivery:
Improve solubility and bioavailability.
Protect fragile drugs from enzymes, pH, immune recognition, and premature clearance.
Control release over minutes, days, months, or even years.
Keep concentrations within the therapeutic window: high enough to work, but below toxic levels.
Reduce off-target exposure in healthy tissue.
Help drugs cross biological barriers or enter specific cells.
Key takeaways:
Drug delivery controls the pharmacokinetic journey of a therapeutic: its dissolution, stability, distribution, targeting, and release rate.
Controlled-release systems replace the peak-and-trough profile of conventional dosing with sustained, predictable concentrations.
Nanoscale carriers, including liposomes, lipid nanoparticles, and polymeric particles, protect fragile cargo and can be engineered to accumulate at disease sites.
For many modern medicines, especially RNA and gene-based therapies, the delivery system is not an accessory; it is the enabling technology.
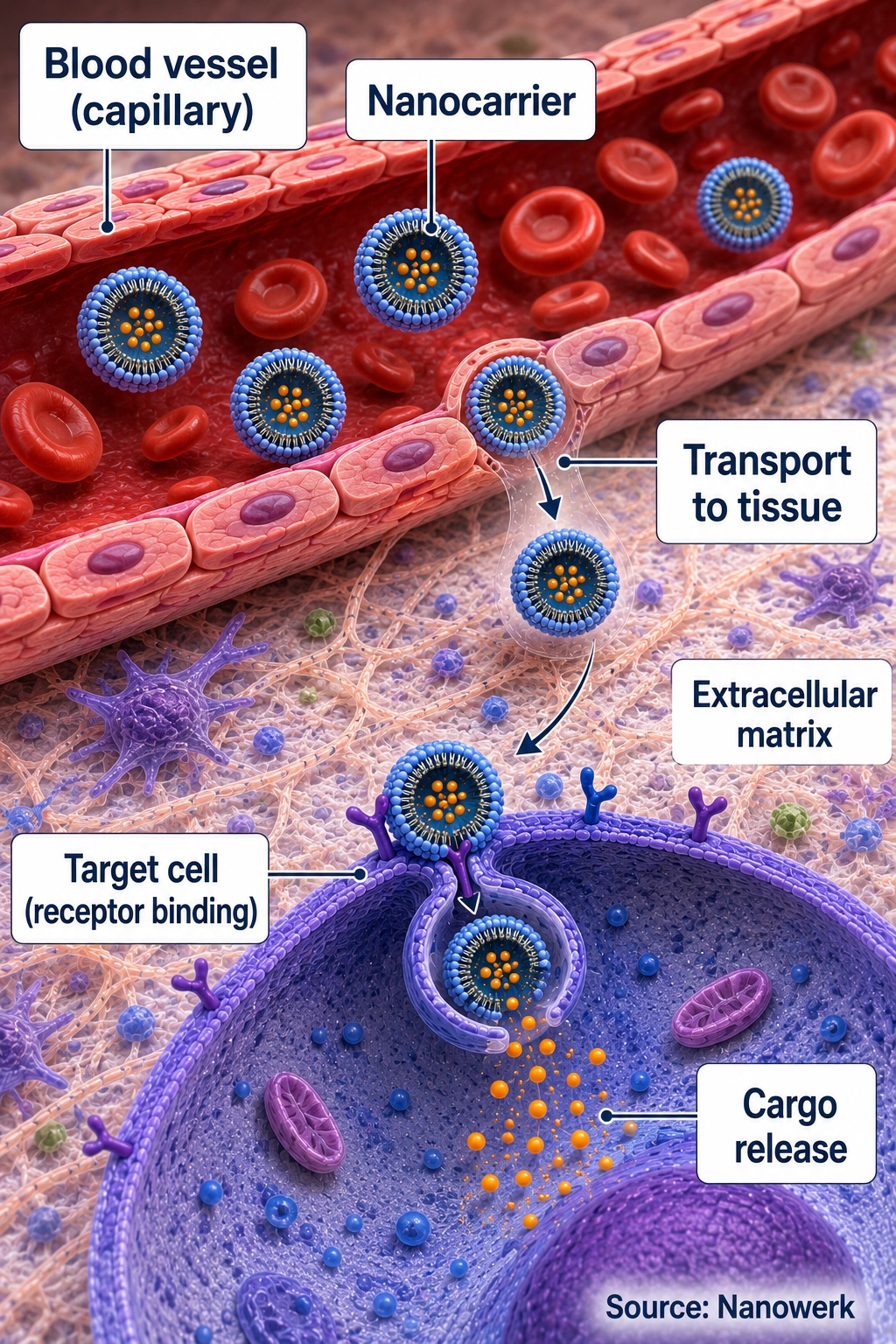
Drug delivery systems such as nanocarriers can protect therapeutic cargo in the bloodstream, help transport it into target tissue, and release the drug near or inside target cells. (Image: Nanowerk)
Why Conventional Dosing Falls Short
The limitations of giving a drug in its free form follow directly from how the body handles foreign molecules. After an intravenous dose, the drug distributes throughout the whole body. Reaching a useful concentration at a small diseased region can therefore mean exposing every other organ to the same compound. For potent cytotoxic agents, this creates dose-limiting toxicity: the maximum tolerable systemic dose is reached before the tumor receives the ideal concentration.
Fragile modern therapeutics make the problem sharper. Therapeutic proteins and nucleic acids such as messenger RNA and small interfering RNA are often degraded by enzymes or cleared rapidly, and many are too large or too charged to cross cell membranes unaided. Monoclonal antibodies pose a different delivery challenge: they can circulate for long periods, but their large size limits tissue penetration and makes intracellular targets difficult to reach. Without appropriate delivery, formulation, or route selection, many biologics and genetic medicines have little oral bioavailability or cannot reach the compartment where they need to act.
Routes of Administration
Drug delivery starts with the route of administration. Oral delivery is convenient but exposes drugs to stomach acid, digestive enzymes, mucus, intestinal transporters, and first-pass metabolism in the liver. Intravenous injection bypasses absorption barriers but exposes the drug or carrier immediately to blood proteins, immune recognition, and rapid clearance. Subcutaneous and intramuscular injections can create depots for slow absorption. Inhaled delivery targets the lung but must navigate mucus and airway clearance. Transdermal patches must cross the skin's tight barrier, while intravitreal injections and implants place medicines directly inside the eye. Each route changes the design problem.
Controlled Release: Taking Charge of the Concentration Curve
The earliest and still most widely used branch of drug delivery is controlled release, in which a formulation governs the rate at which a drug becomes available rather than its destination. The goal is to keep the drug concentration inside the therapeutic window — above the level needed for efficacy and below the level that causes toxicity — for as long as possible from a single administration.
In diffusion-controlled systems, the drug migrates through a polymer matrix or across a rate-limiting membrane, so the geometry and permeability of the material set the release rate. In degradation-controlled systems, the drug is locked inside a biodegradable polymer such as poly(lactic-co-glycolic acid), and it is freed as the polymer erodes by hydrolysis over days to months. Osmotically driven systems use water influx to pump drug out through a small orifice at a near-constant rate. Stimulus-responsive systems release their cargo only when they encounter a trigger, such as the lower pH of a tumor or inflamed tissue, a particular enzyme, or an externally applied signal such as heat or light.
These mechanisms underpin products ranging from once-daily oral tablets to long-acting injectable depots that release a drug steadily for one to six months. They are especially valuable for chronic conditions where missed doses are common.
Biological Barriers a Delivery System Must Cross
Any carrier introduced into the body immediately confronts a sequence of defenses that evolved to exclude foreign particulates. Understanding these barriers is the core of rational delivery design. Within seconds of entering plasma, a nanoparticle adsorbs a layer of proteins known as the protein corona. This coating, rather than the bare particle surface, strongly influences how the body recognizes the carrier.
The mononuclear phagocyte system, with dense populations of macrophages in the liver and spleen, then clears a large fraction of injected nanoparticles. This is why the liver is the organ most successfully reached by many intravenously administered nanoparticles, and why surface coatings that reduce protein adsorption are central to extending circulation time. Immune reactions, complement activation, infusion reactions, and accelerated clearance after repeated dosing are practical concerns for several nanoparticle and PEGylated systems.
A carrier that survives circulation still has to leave the blood vessels and reach the diseased cells. In most healthy tissue the vascular wall is tight, but in many solid tumors and sites of inflammation it is abnormally leaky, allowing nanoscale particles to escape and accumulate. Beyond the vessel wall lie further obstacles: the dense extracellular matrix, the cell membrane, and, for genetic medicines, the endosomal membrane. Endosomal escape is often the central bottleneck for RNA and DNA delivery, because most internalized cargo is trapped and degraded unless it reaches the cytoplasm before the endosome matures into a degradative compartment. Specialized barriers such as the blood-brain barrier, the mucus layer lining the gut and airways, and the tight junctions of the skin add further constraints for delivery to particular organs.
Nanoscale Carriers and Why Size Matters
Operating at the nanoscale, often with carrier diameters from roughly 10 to a few hundred nanometers, gives drug delivery physical levers unavailable to a free small molecule. Particles in this range are large enough to carry a payload and to avoid immediate kidney filtration, yet small enough to circulate through capillaries and sometimes exploit the leaky vasculature of tumors. Their high surface-to-volume ratio provides area for targeting ligands and stealth coatings, while the particle interior shields fragile cargo from enzymes in the blood. Several carrier families have reached the clinic or advanced development, each with a characteristic set of strengths.
Beyond these workhorses, the field uses gold nanoparticles and magnetic nanoparticles for combined therapy and imaging, nanogels and nanocapsules for soft, high-water-content reservoirs, and nanoemulsions for poorly soluble lipophilic compounds. The choice among them is governed by the cargo: a small hydrophobic chemotherapeutic, a fragile protein, and a charged nucleic acid each impose different requirements on encapsulation chemistry, release mechanism, and surface design. The carrier surface is often modified, through surface functionalization, with a hydrophilic polymer such as polyethylene glycol to suppress protein adsorption and prolong circulation.
Passive and Active Targeting
Getting a carrier to accumulate where the disease is, rather than everywhere, is the goal of targeted drug delivery, and it is pursued through two broad strategies. Passive targeting relies on the carrier's size and the abnormal biology of the disease site. The best-known example is the enhanced permeability and retention (EPR) effect: the blood vessels feeding many solid tumors are disorganized and leaky, so circulating nanoparticles seep into the tumor interstitium, while the tumor's poor lymphatic drainage prevents them from being washed out. The EPR effect motivated much of the first generation of cancer nanomedicines, although its magnitude varies substantially between tumor types and is often weaker and more heterogeneous in human patients than in rodent models.
Active targeting adds a molecular recognition step. The carrier surface is decorated with ligands, such as antibodies, antibody fragments, nanobodies, peptides, sugars, or small molecules, that bind receptors over-expressed on target cells. Active targeting generally does not increase the total amount of carrier that reaches the tissue, which is still governed by blood flow and vascular permeability. Instead, it improves binding or uptake into the intended cells once the carrier has arrived. A clinically important variant is endogenous targeting, in which the particle is engineered so that, after it adsorbs specific plasma proteins, the resulting protein corona itself routes it to a particular cell type. The uptake of certain liver-directed lipid nanoparticles by hepatocytes through adsorbed apolipoprotein E is a validated example of this mechanism.
Applications
Cancer therapy
Oncology has historically been the largest single application of nanoparticle drug delivery. Encapsulating a cytotoxic drug in a liposome or polymeric particle can reduce distribution to healthy tissue, lowering characteristic toxicities while maintaining or improving exposure at the tumor. Doxil/Caelyx, a liposomal form of doxorubicin, is a classic example of an approved nanomedicine. The strategy has since extended to combination payloads, carriers that release cargo in response to the tumor microenvironment, and cancer immunotherapy, where delivery systems concentrate immune-stimulating agents in tumors and lymphoid tissue.
Genetic and RNA medicines
The delivery problem is most acute, and its solution most consequential, for nucleic acid drugs. Lipid nanoparticles built around ionizable lipids are the enabling technology behind approved siRNA therapeutics such as patisiran, and the mRNA vaccines Comirnaty and Spikevax are among the largest-volume deployments of engineered nanomedicine to date. The ionizable lipid is nearly neutral in blood but becomes positively charged in the acidic endosome, which promotes the membrane disruption needed for the RNA to escape into the cytoplasm. Carrier design is also a central problem in gene therapy and RNA interference, where non-viral particles are increasingly developed as alternatives to viral vectors.
Vaccines and immunotherapy
Vaccines are also drug delivery systems. The formulation must protect the antigen or genetic blueprint, bring it into contact with the right immune cells, and often provide an adjuvant signal that teaches the immune system to respond strongly. Delivery design influences whether vaccine cargo remains local, drains to lymph nodes, enters antigen-presenting cells, or releases inflammatory signals. This is why lipid nanoparticles, emulsions, polymer particles, and hydrogels are all explored for vaccines and immunotherapies.
Long-acting and localized delivery
Not all delivery innovation is nanoscale. Long-acting injectable and implantable formulations release a drug steadily for weeks to years and have transformed treatment in areas where daily adherence is difficult, including contraception, hormone suppression, antipsychotic maintenance, and treatment of opioid and alcohol dependence. Drug-eluting coronary stents, intravitreal implants for eye disease, and tissue-engineering scaffolds that release growth factors deliver a drug directly at the site where it is needed and keep systemic exposure low. These platforms are an important reminder that drug delivery spans length scales from the molecular to the macroscopic device.
Characterization, Manufacturing, and Quality Control
For nanocarriers, the medicine is not defined only by its chemical ingredients. Size, size distribution, surface charge, shape, drug loading, release kinetics, and manufacturing process are part of the product. Particle size and distribution are measured by dynamic light scattering and nanoparticle tracking analysis, while surface charge is assessed through zeta potential measurement. Drug loading, encapsulation efficiency, and in vitro release profiles must be quantified and shown to be reproducible from batch to batch.
This sensitivity to physical structure is one reason complex nanomedicines can be difficult to scale, regulate, and compare with generic versions. Small changes in mixing, purification, lipid composition, polymer molecular weight, or storage conditions can alter biodistribution and clinical performance. Manufacturing reproducibility is therefore a central scientific and regulatory challenge, not just a production detail.
Challenges and Future Perspectives
Three problems dominate current research. The first is targeting beyond the liver: the same biology that makes the liver easy to reach makes most other organs hard, and reliable delivery to tumors, the brain, the lungs, and immune cells in humans remains only partially solved. The second is the gap between animal models and patients, exemplified by the variable and often modest EPR effect in human tumors, which has made some early efficacy expectations difficult to reproduce in the clinic. The third is manufacturing: nanoscale carriers are sensitive to process conditions, and producing them reproducibly at clinical scale, with appropriate stability and storage, is a substantial engineering undertaking.
The research frontier is moving toward more precise control: stimulus-responsive carriers that release cargo only at the disease site, particles engineered to exploit endogenous protein interactions for extrahepatic targeting, and high-throughput screening and machine learning methods that navigate the large design space of lipid and polymer formulations. Increasingly, the drug and the delivery system are designed together from the start, because for many modern medicines the carrier determines whether the active molecule can work at all.
Frequently Asked Questions
What is the difference between drug delivery and targeted drug delivery?
Drug delivery is the broad discipline of controlling how, where, and when a therapeutic agent reaches and acts in the body, including controlled release, solubility enhancement, and protection of fragile molecules. Targeted drug delivery is a subset focused specifically on concentrating the drug at a chosen tissue or cell type while sparing healthy tissue, usually through passive accumulation or active ligand-receptor binding. Every targeted system is a drug delivery system, but many important delivery technologies, such as oral sustained-release tablets, are not targeted in this sense.
Why do most drug-carrying nanoparticles end up in the liver and spleen?
Once in the bloodstream, nanoparticles adsorb a layer of plasma proteins called the protein corona, which can mark them for recognition by the mononuclear phagocyte system. The liver and spleen are the principal filtering organs of this system and contain large populations of resident macrophages, so a substantial fraction of an intravenous nanoparticle dose is cleared there. Reducing this clearance, often with polyethylene glycol surface coatings, is one of the central engineering challenges in nanoparticle drug delivery, and it is also why the liver is the organ most successfully targeted to date.
How do lipid nanoparticles deliver mRNA vaccines?
A lipid nanoparticle encapsulates fragile mRNA inside a core of ionizable lipids that are nearly neutral in the blood but become positively charged in the acidic environment of a cell's endosome. After the particle is taken up by a cell, this charge change helps disrupt the endosomal membrane and release the mRNA into the cytoplasm, where the cell's ribosomes translate it into the target protein. This delivery system enabled mRNA vaccines such as Comirnaty and Spikevax.
What is the EPR effect in cancer drug delivery?
The enhanced permeability and retention (EPR) effect describes the tendency of nanoscale particles to accumulate preferentially in some solid tumors. Many tumor blood vessels are abnormally leaky, allowing nanoparticles to escape into tumor tissue, while poor lymphatic drainage limits their clearance, so they are retained. The EPR effect underpins the passive targeting of many nanomedicines, although its magnitude varies widely between tumor types and between animal models and human patients.
Is nanoparticle drug delivery only used for cancer?
No. Although oncology has historically dominated the field, nanoparticle and controlled-release delivery systems are used or in development for infectious disease vaccines, genetic medicines such as small interfering RNA and gene therapy, long-acting contraceptives and antipsychotics, ophthalmic implants, and the oral, inhaled, or localized delivery of biologics. The clinical success of lipid nanoparticle mRNA vaccines significantly broadened the perceived scope of the field beyond cancer.